This note is a companion to the Measurement chapter of Global Health Research in Practice, which covers outcome measurement. Here we use a 2026 pancreatic cancer trial to draw out the difference between a surrogate endpoint and the outcome a patient actually cares about.
In late May 2026, a pancreatic cancer result drew the kind of reaction that cancer results rarely get. RASolute 302, a phase 3 trial of the experimental RAS inhibitor daraxonrasib, reported a median overall survival of 13.2 months on the drug versus 6.7 months on chemotherapy—a hazard ratio for death of 0.40, meaning the death rate on the drug was about 60% lower. That is a large effect in any trial, but especially for a disease like metastatic pancreatic ductal adenocarcinoma where there have been few wins.
Reading beyond the headlines, there is a methods lesson here about outcomes and measurement. Daraxonrasib is notable not only for the size of its effect but for the endpoint it shifted.
Three kinds of endpoints
When we say a cancer drug “works,” we are usually pointing at one of three kinds of measurement.
Overall survival (OS) is the endpoint that matters most directly: are patients on the drug alive longer than patients who are not? Every other endpoint is a stand-in for it, and it is the one trials least often wait for, because measuring it means counting deaths, which takes time.
Those stand-ins are surrogate endpoints. In cancer they mostly take two forms:
Tumor response—did the tumor shrink or clear? Overall response rate (ORR), the share of patients whose tumors shrink by a defined amount, is the familiar one; complete remission, minimal residual disease response, and duration of response are variations on the same question. They confirm the drug does something to the tumor, early. Whether that translates into a longer life is a separate question.
Time to an event—how long until the cancer grows, comes back, or spreads? Progression-free survival (PFS), the time until the tumor grows or the patient dies, is the familiar one; disease-free, relapse-free, and metastasis-free survival apply the same idea to different settings. These sit intuitively closer to survival than a tumor measurement does, but a tumor holding still on a scan can still diverge from how long the patient actually lives.
The FDA publishes a running list of the surrogate endpoints it will accept as the basis for approving a drug. In cancer, there are 21 accepted endpoints in adults and 7 in children, almost all are tumor-response or time-to-event measures. Most cancer drugs reach the market on the back of one of these endpoints. A 2019 analysis of 188 oncology approvals between 2006 and 2017 by Chen and colleagues found a surrogate endpoint was the basis for roughly 7 of 10 approvals.
The case for surrogate endpoints
If overall survival is the outcome that matters most, why measure anything else? Because measuring it means waiting for patients to die, and that wait is costly—in time, in trial size, and sometimes in access to a drug that works.
A survival endpoint follows patients until enough of them have died, which can take years in cancers where treatment helps. Surrogate endpoints register earlier: a tumor either shrinks or it does not within the first few scans, and progression usually arrives well before death. Events that accrue sooner let a trial reach a statistical answer with fewer patients and less follow-up. Chen et al. estimated that, after adjusting for how fast trials enrolled and which line of therapy they tested, studies that used progression-free survival as the basis for approval were about 11 months shorter than studies using overall survival, and studies using response rate about 19 months shorter.
Overall survival is also hard to attribute to the drug under study, because it counts death from any cause. A patient who progresses, switches to another therapy, and lives longer because of that next drug still counts as a survivor in the original trial. Crossover, later lines of treatment, and deaths unrelated to the cancer all loosen the link between the drug and the survival curve. A progression or response event is usually recorded while the patient is still on the assigned treatment, which ties it more directly to the intervention.
For the most lethal diseases, an earlier signal also carries ethical weight. When patients have no good options, a credible early readout can reach them sooner. This is the logic behind the FDA’s accelerated-approval pathway, which lets a surrogate stand in for survival on the condition that a confirmatory trial follows.
Each of these arguments is real, and each rests on the same assumption: that the surrogate actually predicts survival. A surrogate earns that standing not by moving with the disease but by being shown to track the outcome patients care about, which is exactly where it can fail.
When surrogate endpoints get it wrong
Bevacizumab (Avastin) in metastatic breast cancer is the cautionary case.
In the E2100 trial, adding bevacizumab to paclitaxel as first-line treatment roughly doubled progression-free survival—11.8 versus 5.9 months, a hazard ratio of 0.60—and raised the tumor response rate from 21% to 37%. Overall survival barely moved: 26.7 versus 25.2 months. The FDA granted accelerated approval in February 2008 on the surrogate endpoint result, on the condition that two trials Genentech already had underway, AVADO and RIBBON-1, confirm the benefit.
When AVADO and RIBBON-1 reported about two years later, both reproduced the progression-free-survival gain and again found no survival benefit, while serious adverse events rose. In July 2010 an FDA advisory committee voted 12 to 1 against the indication; that December the agency’s oncology office formally proposed withdrawing it, and the FDA revoked the indication in November 2011, after Genentech requested a hearing. The agency concluded that women who took the drug “did not live any longer than women who did not receive the drug, and yet were at risk of experiencing severe side effects, including side effects that are unique to this drug and death.”1
The pattern is common. A 2025 review of 791 phase 3 oncology trials found that of the 434 that reported a positive surrogate endpoint, only 43% (185 trials) went on to show an overall-survival benefit.
The RASolute 302 trial
Daraxonrasib is the contrasting case: the trial that moved the surrogate and the survival endpoint together. RASolute 302 was a phase 3, international, open-label trial that randomly assigned 500 patients with previously treated metastatic pancreatic cancer, 1:1, to daraxonrasib or the investigator’s choice of standard chemotherapy. Overall survival and progression-free survival were the dual primary endpoints, prespecified in the RAS G12 subgroup.2 Progression was read by blinded independent central review, and crossover between the arms was not permitted, which keeps the survival comparison clean.
Show code
# Verified against the RASolute 302 primary report (overall population, Results p.4-5).# OS: 13.2 (95% CI 10.0-NR) vs 6.7 (5.8-8.0) mo, HR 0.40.# PFS: 7.2 (95% CI 5.7-7.5) vs 3.6 (2.9-4.2) mo, HR 0.49.ras <-tribble(~endpoint, ~group, ~months, ~lo, ~hi, ~nr,"Overall\nsurvival", "Daraxonrasib", 13.2, 10.0, NA, TRUE,"Overall\nsurvival", "Chemotherapy", 6.7, 5.8, 8.0, FALSE,"Progression-free\nsurvival", "Daraxonrasib", 7.2, 5.7, 7.5, FALSE,"Progression-free\nsurvival", "Chemotherapy", 3.6, 2.9, 4.2, FALSE) |>mutate(endpoint =factor(endpoint, levels =c("Progression-free\nsurvival","Overall\nsurvival")),group =factor(group, levels =c("Daraxonrasib", "Chemotherapy")),# x position of each dodged bar, so error bars/labels line up by handxpos =as.numeric(endpoint) +ifelse(group =="Daraxonrasib", -0.175, 0.175) )ggplot(ras, aes(x = endpoint, y = months, fill = group)) +geom_col(position =position_dodge(width =0.7), width =0.6) +# 95% CIs with a reached upper boundgeom_errorbar(data =filter(ras, !nr),aes(x = xpos, ymin = lo, ymax = hi),inherit.aes =FALSE, width =0.10,color ="grey25", linewidth =0.5) +# daraxonrasib OS: lower cap + upward arrow (upper bound not reached)geom_errorbar(data =filter(ras, nr),aes(x = xpos, ymin = lo, ymax = lo),inherit.aes =FALSE, width =0.10,color ="grey25", linewidth =0.5) +geom_segment(data =filter(ras, nr),aes(x = xpos, xend = xpos, y = lo, yend =16.7),inherit.aes =FALSE, color ="grey25", linewidth =0.5,arrow =arrow(length =unit(0.18, "cm"), type ="closed")) +geom_text(aes(x = xpos, y = months, label = months),inherit.aes =FALSE, hjust =-0.3, size =3.6, color ="grey20") +scale_fill_manual(values =c("Daraxonrasib"= ghr_blue,"Chemotherapy"= ghr_orange)) +expand_limits(y =17.5) +labs(title ="A randomized comparison on survival itself",subtitle ="Median months with 95% confidence intervals; hazard ratio 0.40 for death, 0.49 for progression",x =NULL, y ="Median months", fill =NULL) +theme(legend.position ="top",panel.grid.major.x =element_blank(),panel.grid.minor.x =element_blank())
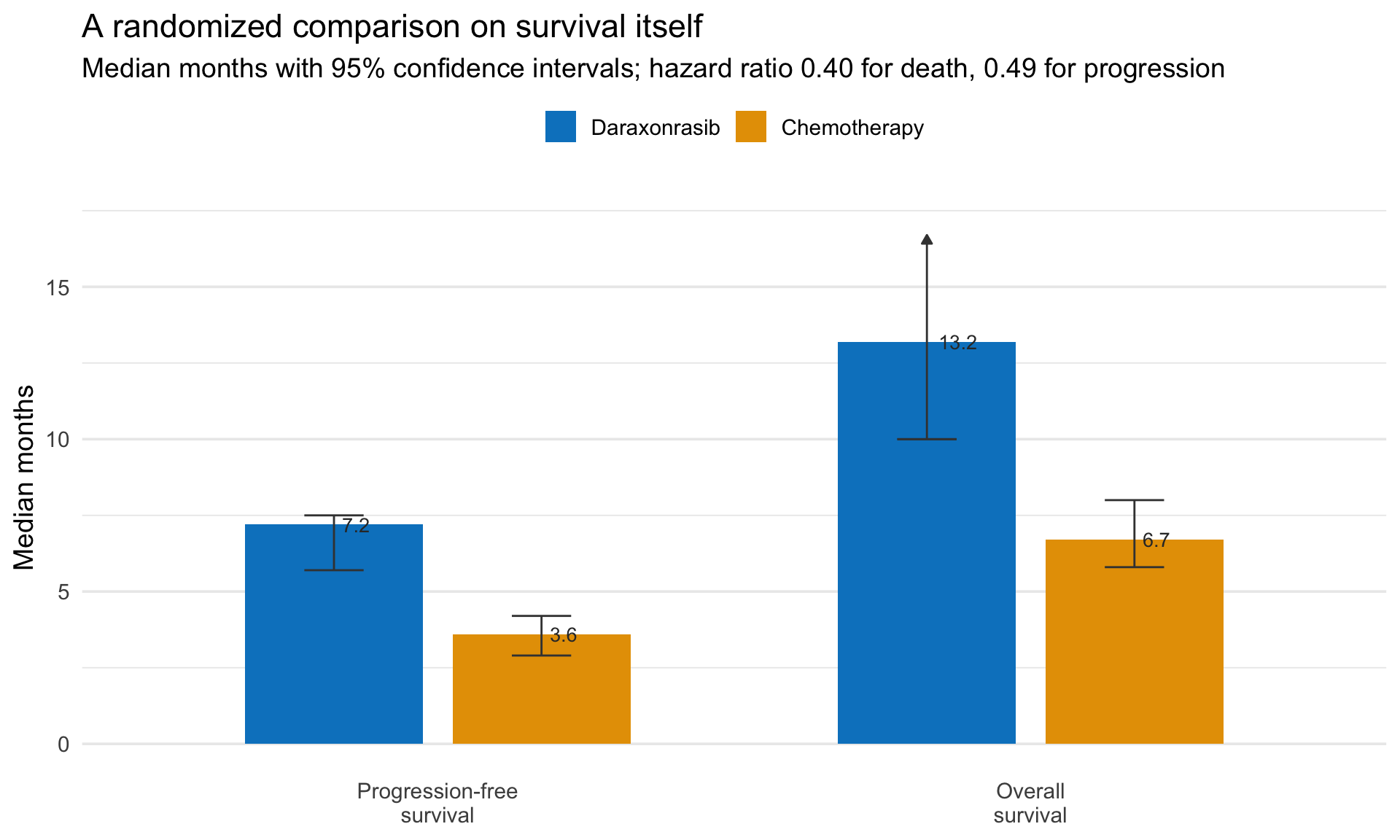
Figure 1: RASolute 302, overall population (N = 500): median overall and progression-free survival, daraxonrasib versus chemotherapy, with 95% confidence intervals. The upper bound of the daraxonrasib overall-survival interval was not reached at the data cutoff (shown as an upward arrow). Source: O’Reilly et al., New England Journal of Medicine, 2026 (DOI 10.1056/NEJMoa2605555).
The endpoints moved together. Overall survival roughly doubled (13.2 vs 6.7 months, HR 0.40), progression-free survival followed (7.2 vs 3.6 months, HR 0.49), the objective response rate was about three times higher (32% vs 11%), and patient-reported pain and quality of life both took longer to worsen on the drug than on chemotherapy.3 These endpoints are coherent, not independent. When response, progression, survival, and patients’ own reports all move the same way in one randomized comparison, the result is hard to dismiss as an artifact of any single measure. But they are correlated readings of the same patients, not separate lines of evidence with their own biases, so the consistency strengthens confidence without standing in for replication in another trial.
Key takeaways
Daraxonrasib moved the endpoint that matters. RASolute 302 reported a median overall survival of 13.2 versus 6.7 months, a hazard ratio of 0.40, in a randomized trial—for metastatic pancreatic cancer, a disease with few wins. The result is notable not only for its size but because it landed on overall survival itself rather than a stand-in for it.
Overall survival is the outcome; the rest are stand-ins. Response rate and progression-free survival read out earlier and substitute for overall survival, which is why they are the basis for most cancer drug approvals—roughly 7 in 10 in Chen et al.’s analysis.
Surrogates buy speed but only pay off if they predict survival. Earlier endpoints make trials smaller and faster, tie the result more cleanly to the drug, and can move a treatment to patients who have no other options sooner. The catch is the link to survival, which can fail: bevacizumab roughly doubled progression-free survival in metastatic breast cancer without lengthening overall survival, and the FDA withdrew the indication. Across 791 modern oncology trials, a surrogate gain reached overall survival less than half the time.
Footnotes
U.S. FDA, Center for Drug Evaluation and Research, “Regulatory Decision to Withdraw Avastin (bevacizumab) First-line Metastatic Breast Cancer Indication,” Office Director memorandum, BLA 125085, December 15, 2010. The memo proposes withdrawal—recording the February 22, 2008 accelerated approval, the failed confirmatory trials, and the 12-to-1 ODAC vote—and the Commissioner’s final decision revoking the indication followed in November 2011.↩︎
The RAS G12 subgroup is the patients whose tumors carried a RAS mutation at codon 12, by far the most common driver mutation in pancreatic cancer; it made up about 92% of the trial. Naming that group in the protocol as the primary-analysis population, before any results were in, is what prespecified marks: the comparison was committed to in advance rather than chosen afterward to fit the data.↩︎
One caveat on the survival number: my understanding is that it comes from the first of two planned interim analyses. At the data cutoff the median follow-up was 8.5 months, shorter than the 13.2-month median survival the trial reports, and the final analysis is still to come. That immaturity is why the upper confidence bound on survival was not reached, and it means the estimate can still move as more deaths accrue. The same caution cuts the other way for bevacizumab: the FDA later judged that E2100’s progression-free-survival result, also read at an interim analysis, may have been a “random high.”↩︎